

(Original Post Date: 9/22/22)
To derive strengthening benefits from exercise, it's crucial that the exercise is performed at an appropriate intensity. There are various methods to increase intensity; commonly, we add weight or increase the number of repetitions. But what exactly constitutes 'appropriate intensity'? Research indicates that approaching muscular failure each set suggests the exercise was intense enough to provide a benefit1. But what does that look like?
"How much weight should I lift? When should I consider adding weight?”
These are excellent questions, and addressing the first one can be relatively straightforward: for example, squat 100 pounds for 4 sets of 5 reps. And this can be effective! The numbers are clear, and it can be easily progressed by adding weight, reps, or sets. However, answering the second question is a bit more difficult. There's no one-size-fits-all framework. We can't simply say, 'Follow this exercise routine for 3 weeks, then add 10 pounds and continue for another three weeks,' because while it might work for some, it might not for others. Everyone adapts differently and some people may be ready for significant progression while others may even need to regress and do less. This is where autoregulation comes into play.
Autoregulation involves adjusting training based on your performance to facilitate improvement at your optimal pace. This can be done using two common autoregulatory strategies: Rate of Perceived Exertion (RPE) and Repetitions in Reserve (RIR)2. RPE asks, 'How hard did that exercise feel?' This is typically graded on a scale of either 1-10 or 6-20, where 10 or 20 indicates an all-out maximal effort, with higher numbers representing greater difficulty. Personally, I find the 1-10 scale more intuitive than the 6-20 scale, the key is using the one that is most intuitive to you.
RIR, on the other hand, asks, 'How many more reps could I do before I could not do any more?' For instance, if I squat 8 times and at the end of the set I believe I could perform 2 more reps, but not a third, then I have 2 reps in reserve.
I find RIR to be more straightforward than RPE. However, they are closely correlated3, and RPE can be easily calculated if you know your RIR by simply subtracting your RIR from 10. In the previous example, since my RPE is 8, my RIR would be ~2 more reps.
Understanding these metrics is useful, but how does it help in determining the 'appropriate intensity' for an exercise? If we derive strengthening benefits from nearing muscular failure, then we will also benefit from training to a higher RPE (or lower RIR). Therefore, to make further progress the goal of exercise is to reach an RPE of 7-8 (or 2-3 RIR) during every set of a strength training exercise. This implies approaching failure but not actually reaching it.
Why not go to 10 RPE or 0 RIR? Generally going to complete failure corresponds with more soreness and fatigue, which means you typically cannot get as many total sets in during a given time frame, as more rest is likely needed. It isn’t necessary to go to complete failure in order to achieve strength improvements.
However, this is not an exact science. Both RPE and RIR are subjective assessments based on how we currently feel. They may not always be accurate, but with experience, this process becomes more intuitive. Sometimes, it can be enlightening to challenge yourself. If you're nearing the end of a set of squats and you believe you could only manage 2 more reps before reaching failure, you could occasionally try to push beyond that to test your guess. You may surprise yourself with how many more reps you can actually perform!
"But what about when I have pain?”
As performance physical therapists, we often deal with individuals experiencing pain, so this is a common concern we face. You might be aware that you're capable of performing more reps of an exercise, but you also know that pushing to a 7-8 RPE (2-3 RIR) would result in pain. Fortunately, the solution is relatively simple: you can utilize the Numeric Pain Rating Scale (NPRS). This is the classic 0-10 pain scale we're all familiar with, where 0 signifies no pain and 10 represents the worst pain imaginable.
Typically, we advise pushing into a bit of discomfort during the rehabilitation process (though this depends on the specific injury you're recovering from; for example, with stress fractures, we want to avoid any pain, but with tendinopathies, some mild discomfort is usually acceptable). We generally recommend not exceeding 3-4 out of 10 on the NPRS, as long as this discomfort doesn't persist for more than 2-3 hours after finishing the exercise and is back to baseline by the next day.
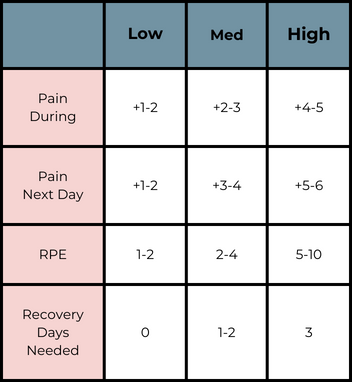
Finally, let's bring it all together! You can gauge the pain experienced during an exercise (NPRS), the intensity of the exercise (RPE or RIR), and your pain the following day (NPRS). Then, using these three metrics, and the chart provided below, you can determine whether it's advisable to perform that activity again, if you should wait a day or two before repeating those exercises, or if you need to wait three days before attempting them again4.
Check out this brochure I made to help clarify any points from this blog.
References
- Androulakis-Korakakis P, Fisher JP, Steele J. The minimum effective training dose required to increase 1RM strength in resistance-trained men: a systematic review and meta-analysis. Sports Med. 2020;50(4):751-765. doi: 10.1007/s40279-019-01236-0.
- Helms ER, Kwan K, Sousa CA, Cronin JB, Storey AG, Zourdos MC. Methods for regulating and monitoring resistance training. J Hum Kinet. 2020;74:23-42. doi: 10.2478/hukin-2020-0011.
- Lovegrove S, Hughes LJ, Mansfield SK, Read PJ, Price P, Patterson SD. Repetitions in reserve is a reliable tool for prescribing resistance training load. J Strength Cond Res. 2022;36(10).2696-2700. doi: 10.1519/JSC.0000000000003952.
Silbernagel KG, Crossley KM. A proposed return-to-sport program for patients with midportion Achilles tendinopathy: rationale and implementation. J Orthop Sports Phys Ther. 2015;45(11):876-86. doi: 10.2519/jospt.2015.5885.